
Facing Fears and Phobias in Therapy
By Darrell Provinse, MA, LPC, NCC
Because we, at ACCS, use a multi-factorial approach to counseling, we use an integrative model in dealing with anxieties, phobias, and PTSD. This includes traditional cognitive interventions, as well as gradual exposure and systematic desensitization, coupled with advanced relaxation techniques, and, as the situation merits, eye movement desensitization and reprocessing, neuro-linguistic programming, and cognitive process therapy. This allows the therapist to address the biology of fear, as well as the thought process, the neurological process, and the behavioral process, which together produce better traction and long-term results.
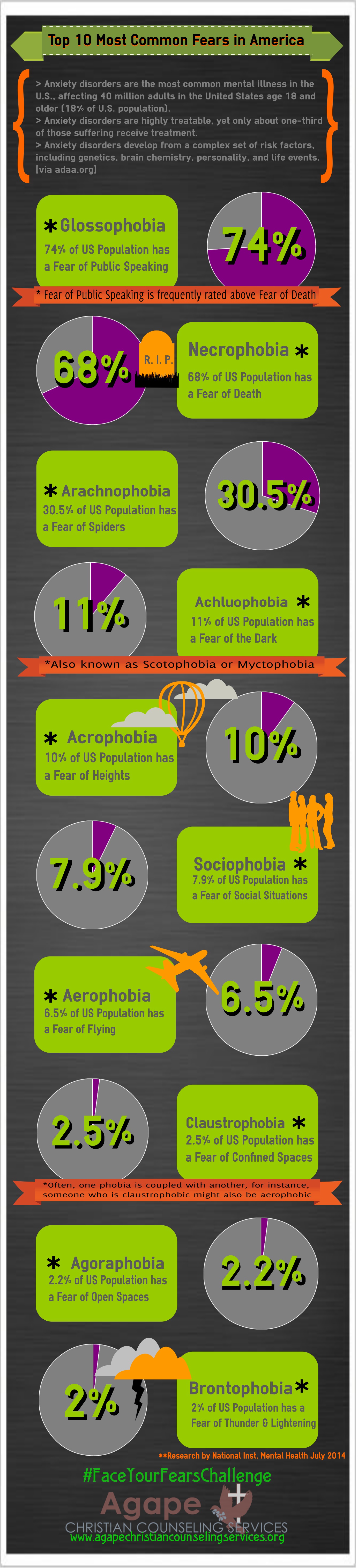 Cognitive interventions typically include getting more factual information through researching statistics or carefully examining the truth of our beliefs. These things might include for example, the statistics regarding airplane safety or the potability of drinking water or what snakes are venomous, etc. These things in and of themselves are helpful but typically are not sufficient to fully dispel a phobia or anxiety that has a stronghold in a person’s thoughts and life. It does, however, provide a foundation and an alternative to the scripts that have been played over and over in our minds when we are beset by a phobia or a profound anxiety.
Cognitive interventions typically include getting more factual information through researching statistics or carefully examining the truth of our beliefs. These things might include for example, the statistics regarding airplane safety or the potability of drinking water or what snakes are venomous, etc. These things in and of themselves are helpful but typically are not sufficient to fully dispel a phobia or anxiety that has a stronghold in a person’s thoughts and life. It does, however, provide a foundation and an alternative to the scripts that have been played over and over in our minds when we are beset by a phobia or a profound anxiety.
The next step in cognitive intervention is to dispute the faulty thinking or scripts, that which we gravitate toward and rehearse in our minds, and identify the part that is untrue, dispelling that and replacing it with fact and truth. As part of that process, we are able to also identify the elements of truth that are interwoven with faulty beliefs as there can be a basis for some level of fear response with regard to heights, snakes, spiders, germs, etc. The problem typically is not that there is a fear response, but that the response is disproportionate and debilitating. By taking what is true and rendering it proportionate, and disputing and discarding what is not true, we then have a rational basis for addressing what by definition is irrational, and that adds to the intensity of the feeling.
The relaxation techniques that we implement at Agape Christian Counseling Services, would not be entirely unfamiliar to many people who have either studied therapeutic interventions or have received them. The way that we do it however, tends to be a little bit more involved and a little bit more advanced than what is typically done in other counseling environments. The process that we use is one of deep and rhythmic breathing and tightening and relaxing of muscles, but then is taken to another level. The reasons for the techniques that we implement are many; they include classical conditioning.
As individuals, twice a day, every day, practice the relaxation techniques that we teach, they are conditioning themselves to be able to relax on cue. For many people, that seems implausible and out of reach at first, but over time, a person is able to recognize at a conscious level those things that are more within their control, but they are also conditioning themselves on an unconscious level to respond quickly and on a behavioral and even at a biological level. It also reduces the effect of fatiguing muscles where people typically will carry anxiety and stress, namely areas of the body such as the neck, shoulders, back, etc. When those muscles are fatigued, it becomes more difficult for individuals to stay tensed unconsciously.
Similarly, by tensing and releasing the muscles and being more aware of breathing and heart rate, we become more aware when we are tense or carrying greater anxiety than what people typically would. By being more aware, it allows us to examine the process and even some of the antecedent triggers. It also allows for more oxygen to get into our system and into our brain. It stimulates a release of endorphins and also has been found to increase the levels of serotonin that the brain produces. It serves as biofeedback, in that, as we become more proficient in the relaxation techniques, we also become more proficient in being able to consciously control things such as breathing, heart rate, etc. and by consciously modulating those, we are able to deactivate the sympathetic nervous system (the fight or flight response). With that in place, we will often use gradual exposure and systematic desensitization. That is where we use the stimulus, whether it be via mental imagery, viewing pictures, or having the stimulus presented in vivo, to begin the process of experiencing to some degree proximity of the phobic or anxiety producing stimulus.
Typically, what will happen is that the client will begin by picturing the triggering stimulus and, when they have a biological response of stress or anxiety or when they have a thought of panic or fear, the therapist will pause the imagery and they will collaborate to slow the client’s breathing and heart rate and return to an appropriate level of systemic arousal. The next step might be the presentation of pictures or videos, or in the case of snakes or spiders, seeing the stimulus from across the room, in a cage or terrarium. The exposure therapy would continue gradually and at a pace that is challenging but not overwhelming for the client.
Cognitive process therapy is especially helpful in use with trauma. It is one where the traumatic event is approached in a controlled and safe way, through a verbal or mental rehearsal of the event with the therapist, as well as in writing. As the thoughts, feelings, etc. are processed, the questions of how did that affect your sense of self, your sense of safety, your beliefs about the world, your beliefs about God, etc. are then processed in order to give context to the current belief system and the resulting behaviors and responses. Over time, and repeated processing of those events, the emotional response typically diminishes, which allows for a modification of those catastrophic beliefs as well.
Neuro linguistic processing and EMDR are both systems by which a stronger neural pathway from the mid-brain, which is highly associated with emotional response, is in better communication with the executive functioning part of the brain, primarily the prefrontal and to some extent the supraorbital cortex. Typically, when one has a fear producing or trauma producing event, it activates the amygdala which is part of the limbic system in the midbrain, which then triggers a release of cortisol in the brain and adrenaline in the body. It evokes memories to be retrieved from the hippocampus that are consistent with that feeling of fear or panic, which then causes the individual to re-experience past fear and trauma in the present, sometimes multiple fears or traumas all at once. In an emergency, the cingulate gyrus, which is associated with transitioning from one thought or event within the consciousness to another, will lock down and prevent that transition because it is still operating as if the threat is very real and present.
In neuro-linguistic programming and eye movement desensitization and reprocessing (EMDR), various cortical structures of the brain are implemented which then necessarily reduce the amount of attention and energy which can be recruited by the midbrain. It allows for more global processing of the fear, the trauma, both in the present and in the past, and allows the individual to be able to be in the presence of what historically was an anxiety or phobic producing stimulus and not experience it at the same level of emotion.
As part of the integrative approach to fears and anxieties, we also take into account avoidant behaviors. Typically, when we avoid something, whether it is in our thoughts or in vivo, it tends to gain in its power. The more we avoid something that produces stress in us, the more we tend to believe that it is something to be feared and beyond our control. We give it power without knowing it. It’s like a schoolyard bully– the more you give it, the more it will demand. In fact, often, the main reason to address phobias such as arachnophobia, agoraphobia, etc. is not because it impairs our functioning on a daily basis, but, more, because it affects how we define ourselves as individuals. The more we give in to fear, the more we see ourselves as fearful or weak or controlled by our feelings, rather than by faith and what we know is true.
By facing and overcoming our fears, we then are able to define ourselves differently as people who are capable, confident, courageous, etc. Therefore, part of the work we do in addressing a phobia or anxiety, is to find ways to accommodate our fears rather than conquer them and change those behaviors. As an individual experiences themselves taking steps forward in their thoughts and ultimately in their actions, that in itself becomes empowering and gives courage and encouragement to proceed. Often the crescendo is a graduating event, whether holding the phobic stimulus in question, or in the case of public speaking, seeking out an event where one can face what, as it turns out, more people fear than death itself.
That does not mean that, with that event, all fear is immediately dispelled, but it does introduce a paradigm of victory, rather than defeat, and of courage, rather than timidity. Often that celebratory event becomes a milestone or landmark in the person’s life to which they can refer and from which they can draw strength as other situations present themselves.



2 Comments
Lois
I’m highly inspired
admin
We are so glad!